Crack vs. Cocaine: A Clinical Comparison for Substance Use Professionals

A clinical perspective on the two forms of cocaine — and why the distinction between them matters for assessment, risk, and treatment planning.
By Benjamin Zohar, NCACIP — Nationally Certified Advanced Clinical Intervention Professional | ISSUP New York Network Moderator
Medical Review: Brandon McNally, RN
Few substance-use terms are conflated as often as "crack" and "cocaine." For substance use professionals, the distinction is not academic: the same active drug, delivered by two different routes, produces meaningfully different patterns of onset, use frequency, and dependence — and carries a distinct legal and historical legacy that continues to shape the populations clinicians serve. This article summarizes the clinical and practical differences for professionals, families, and individuals seeking to understand them.
Same Drug, Two Forms
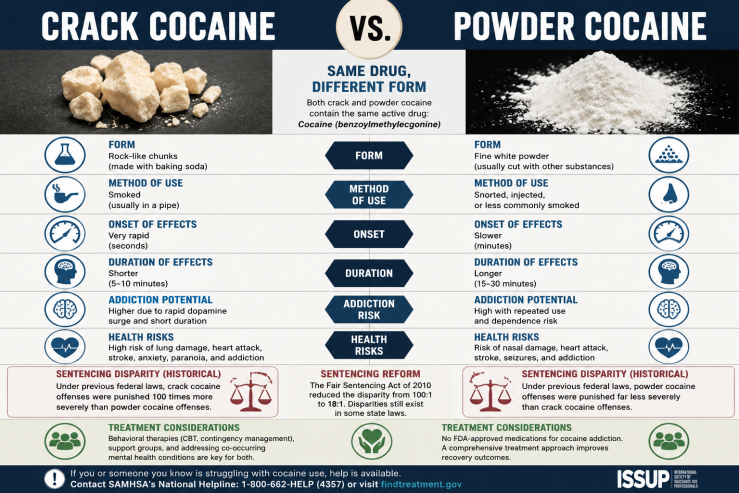
Crack and powder cocaine are derived from the coca plant and contain the same active stimulant. The defining difference is chemical form. Powder cocaine is cocaine hydrochloride, a water-soluble salt that is typically insufflated (snorted) and occasionally injected. Crack cocaine is the freebase form, prepared as solid "rocks" that are smoked, delivering the drug to the brain within seconds.
This single difference — route of administration — accounts for most of the clinically relevant distinctions between the two. The pharmacology of the active compound is the same; the kinetics of delivery are not.
Onset, Duration, and Why It Drives Risk
Smoked crack reaches the brain almost immediately and produces an intense high lasting roughly 5 to 10 minutes. Snorted powder cocaine has a slower onset (a few minutes) and a longer duration (roughly 15 to 30 minutes). The rapid, brief, intense high characteristic of crack tends to promote a compressed cycle of repeated dosing, which reinforces compulsive use more quickly than the slower curve of insufflated cocaine.
This is the core reason crack is frequently associated with a higher risk of rapid dependence — not because it is a "different" or inherently stronger drug, but because the delivery route changes the reinforcement pattern. Both forms are highly addictive, and powder cocaine use disorder remains serious and prevalent.
For a detailed, public-facing breakdown — including a side-by-side comparison of onset, duration, effects, and addiction potential — see this clinical comparison of crack vs. cocaine from Long Island Rehab Helpline & Crisis Intervention.
Clinical and Health Considerations
Because crack and powder cocaine share an active compound, their cardiovascular and neurological risk profiles overlap substantially: elevated heart rate and blood pressure, risk of myocardial infarction and stroke even in young and otherwise healthy individuals, arrhythmias, seizures, and the potential for stimulant-induced psychosis. Overdose risk increases with dose and with co-use of alcohol or opioids.
Route of administration introduces form-specific harms. Chronic insufflation of powder cocaine is associated with nasal damage up to and including septal perforation. Smoking crack is associated with pulmonary injury and respiratory complications. Any injection route adds infection and bloodborne-disease risk. Clinicians taking a history should document route, frequency, and co-use rather than recording "cocaine" as an undifferentiated category.
The Sentencing Disparity: Clinical Relevance of a Legal History
The crack–powder distinction carries a legal legacy that directly shaped the demographics of who was criminalized for cocaine use. Under the Anti-Drug Abuse Act of 1986, federal law applied a 100:1 sentencing ratio between crack and powder cocaine — 100 times as much powder was required to trigger the same mandatory minimum as crack. The disparity was widely criticized for its disproportionate impact on Black communities.
The Fair Sentencing Act of 2010 reduced the ratio to 18:1, and the First Step Act of 2018 made those reductions retroactive. The disparity has narrowed but has not been fully eliminated at the federal level. For clinicians, this history is relevant to understanding the criminal-justice involvement, stigma, and structural barriers that many clients presenting with crack-related histories have experienced.
Treatment Considerations
There are no FDA-approved pharmacotherapies specific to cocaine or crack use disorder; the evidence base centers on behavioral and psychosocial interventions, with medical support during acute withdrawal. Approaches with clinical support include cognitive behavioral therapy, contingency management (among the better-supported interventions for stimulant use disorder), the Matrix Model, and structured residential or intensive outpatient programming for more severe presentations, alongside peer support such as Cocaine Anonymous and SMART Recovery.
While withdrawal from cocaine is rarely physically dangerous in the manner of some other substances, the psychological withdrawal — profound craving, depression, fatigue, and anhedonia — is a primary driver of relapse and warrants clinical attention and follow-up. Families navigating this often benefit from professional guidance; structured treatment navigation on Long Island can help connect a person to the appropriate level of care. Treatment planning should account for route of use, co-occurring substance use, and the psychosocial context, including any criminal-justice involvement.
Resources for Individuals and Families in New York
For individuals and families in New York State seeking help with cocaine or crack use, treatment navigation services can connect people to appropriate levels of care. Resources include:
- Long Island Rehab Helpline & Crisis Intervention — Treatment navigation and crisis support for Long Island and the greater New York City area.
- Every1 Center — Addiction treatment navigation serving the Capital Region and Hudson Valley.
- Hudson Valley Addiction Treatment Center — Treatment resources for the Hudson Valley region.
- Intervention NY — Professional intervention services throughout New York State.
The SAMHSA National Helpline is available 24/7 at 1-800-662-4357 for free, confidential treatment referrals and information. Anyone in immediate crisis can call or text 988 (Suicide & Crisis Lifeline).
Conclusion
Crack and powder cocaine are two forms of one drug, separated chiefly by chemical form and route of administration. Those differences drive distinct patterns of onset, use frequency, and dependence risk, and they sit atop a legal history that has shaped the populations clinicians serve. For substance use professionals, precise assessment — documenting form, route, frequency, and co-use rather than a generic "cocaine" label — supports more accurate risk evaluation and treatment planning.
About the Author
Benjamin Zohar, NCACIP is a Nationally Certified Advanced Clinical Intervention Professional and ISSUP New York Network Moderator with over a decade of experience in addiction treatment navigation and crisis intervention. He operates a network of treatment navigation and placement services across New York State, including Long Island Rehab Helpline & Crisis Intervention, Every1 Center, Hudson Valley Addiction Treatment Center, and Intervention NY.
Medical Reviewer: Brandon McNally, RN, provides clinical accuracy review for published content.
References
- National Institute on Drug Abuse. Cocaine DrugFacts.
- U.S. Drug Enforcement Administration. Cocaine drug fact sheet.
- United States Sentencing Commission. Reports on cocaine and federal sentencing policy.
- Fair Sentencing Act of 2010; First Step Act of 2018.
- Substance Abuse and Mental Health Services Administration (SAMHSA). Treatment resources for stimulant use disorder.
This article is intended for educational and informational purposes for addiction professionals and the general public. It does not constitute medical advice. Individuals concerned about cocaine or crack use should consult a qualified healthcare professional or contact the SAMHSA National Helpline at 1-800-662-4357.